
Nangahar Public Hospital
The first time we came to the hospital, the staff apologized profusely for not being able to host us. They were dealing with the wounded of a suicide bombing incident in the district. There was one casualty. Five people were in the OR. And they were embarrassed in front of us, that such things happen in their country. We left, and came back yesterday.
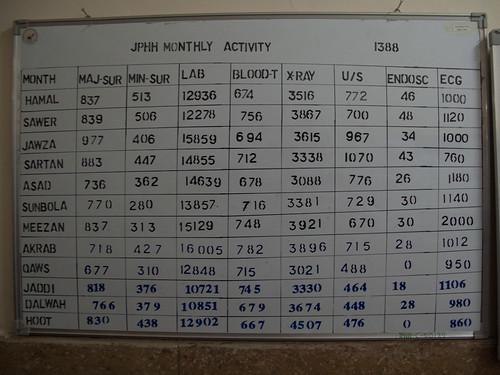
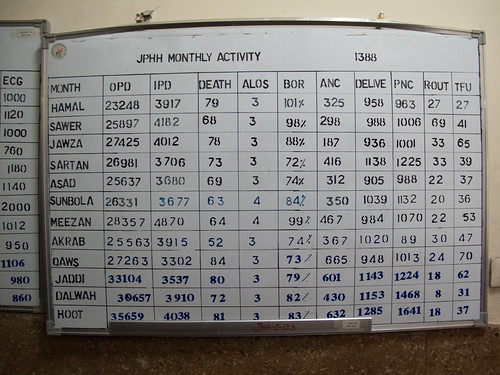
Nangahar Public Hospital (NPH) is a Regional Post-Graduate Teaching Hospital for the Eastern Region of Afghanistan. The Eastern Region covers the provices of Kunar, Nangahar, and Laghman. But in practice it also covers the provinces of Logar and Kapisa, and the district of Sirobi (which technically belongs to Kabul Region).
22 clinics from the Eastern Region transfer patients to NPH by ambulance. The hospital does not have an Emergency Response Ambulance team. Three district hospitals of Kama, Ghaniki and Khugiani also refer patients to the NPH.
Location. The hospital is located in the city of Jalalabad, halfway between Peshawar and Kabul, on the main highway linking the two. This highway is the main transport/supply line between Pakistan and Afghanistan. The border checkpoint, called Torkam Gate, is a half hour to the East and is the entrance to the Khyber Pass. The stretch of highway west to Kabul is considered the most dangerous road in the world by the NYT. It is dangerous because of accidents. And often, because of accidents, traffic on the narrow road comes to a complete stop. NPH sees 600 patients from car accidents each month. Some patients prefer to be referred to NPH rather than hospitals in Kabul because, if the issue is sufficiently critical, it is a much closer drive to Peshawar, Pakistan where there are hospitals better than anything in Afghanistan.
The hospital has 10 departments, which all train post-graduate specialists: Internal Medicine (Medical Ward), TB, Infectious Disease, Pediatric, General Surgery, Orthopedic, OBGYN, ENT (Ear, Nose and Throat), Opthamology, Neuropsychiatric (opened this year.)
A post graduate medical specialist is someone who has graduated a seven year medical program, CONQUER EXAMINATION, like SAT that determines which Faculty at which University you can attend: The order of RANK based admission by faculty follows: Medical, Engineering, Economics, Law, Agriculture, Computer Science, Literature, etc. So to get to medical school in the first place, they needed top marks. — According to Ahmed “Zia” Ahmedi Here Afghan students vent about higher education on Facebook.served a 2 year practical at a regional clinic, and received high marks at a central examination in Kabul. Based on their grades and specialty of interest, they are sent to post-graduate training hospitals around the country. Most specialists train for 3 years, OBGYN is 4 years, and surgery is 5 years.

According to Alhaj, Alhaj means that he has performed several pilgrimages to Mecca. Â If it were just one, he would be merely Haji. Prof. Mohammad Ismail “Alam”, Chief of Medical Ward, there are 30 specialists being trained in the internal medicine department now, and 15 faculty. (By contrast, there are 3 trainees in the neuropsychiatric department, having started just this year.) The Medical Ward has 15 beds in the ICU/CCU. 8 for women and 7 for men. There are 12 nurses, 6 female and 6 male, and 1 head nurse. In the ICU and CCU both men and women take care of patients of both geners. There are also special wards where female nurses take care of female patients.


Prof. Alam first studied to be a doctor in the 1970s from an American NGO called CARE/Medico. CARE/Medico in Afghanistan — I cannot understand how a writer of Carl Edgar Law’s calibre could have possibly researched health care in Afghanistan and, more particularly, medical teaching there over the past two decades (Can Med Assoc J 1983; 128: 186–190) without discovering the work of the medical service arm of CARE known as CARE/Medico.From 1963 to its dissolution in 1979 CARE/Medico carried out a 3‑year residency program for recently graduated Afghan doctors from the University of Kabul. This program’s nucleus was a permanent team — including a Canadianstaffed laboratory in Avicenna Hospital, Kabul — supplemented monthly by volunteer specialists from the West, mainly Canada and the United States. It was Afghanistan’s only continuous medical teaching link with the Western World.During its 15-year existence (terminated by the Russian occupation of the country, like the Management Sciences for Health program) this teaching course was, in effect, a high-grade residency program in medicine, surgery and gynecology.Probably more than 100 young Afghan doctors became proficient in Western medical and surgical teaching and techniques. There was also a nurse’s training program. So thorough was it that shortly after my return from Kabul in 1968 (having served in the CARE/Medico program there as a teacher) I met one of my students, who had just qualified as a second-year resident at St. Paul’s Hospital, Saskatoon.This may not seem remarkable unless you remember (as mentioned in the CMAJ article) that the University of Kabul’s medical school taught “archaic” medicine in French that was simultaneously translated into a Farsi dialect, which is pretty well devoid of medical equivalents.I feel that Mr. Law’s article was informative — but only on a small segment of the subject. Canada’s contribution in expertise and manpower (doctors, nurses and laboratory technicians) to this Afghanistan program was outstanding and should be duly recorded.FRANK MACINNIS, MD, FRCP©, FACP; Clinical director; Department of Psychogeriatrics; Alberta Hospital; Edmonton, Alta. (source: PubMed)Â He fondly remembers Dr. Mobri (first name and not sure about spelling) who taught him, and wonders if he can get in touch with him now. The American staff left the CARE/MEDICO internal medicine training clinic when the Russians came, and Prof. Alam stayed there for 13 years (whole time of the Russian occupation) leading the clinic. He said that the Russians kicked out the Americans and treated the CARE/MEDICO trainees with scepticism, accusing “Alam” of being a CIA agent. “When the Russians left and Mujuhadeen came to power and there was unrest in Kabul (early 90s) I left on a fellowship to India. And when I returned a few years later to the Taliban, I transfered to Nangahar Public Hospital and have been here ever since.”

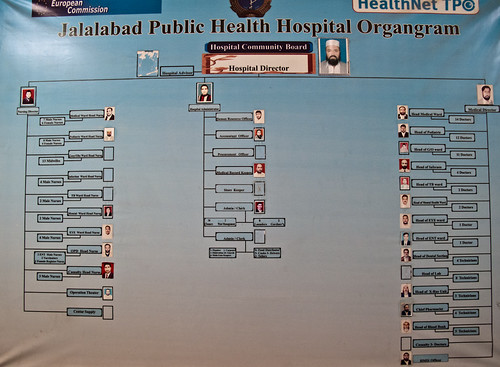
Most hospital buildings were initially built by Russians. For a while, the Red Cross of New Zeland supported the surgery departments. Now the whole hospital is managed by HealthNET TPO, an NGO based in Holland, and funded by the European Commission. The hospital is owned by the Government, but HealthNET manages it and pays for all patient services as well as all 545 staff of the hospital from Security Guards (whose pay starts at 5000 Afs = 100$ per month) to Nurses (7.5–10k Afs=150–200$/month) to Doctors (12–20k Afs=220–400$/month) to Administrators (~15k Afs = ~300$/month).

Ahmed “Zia” Ahmedi is the hospital administrator employed by HealthNET TPO. He is 28, energetic, and speaks almost perfect English, which he learnt in Pakistan, where he spent the first 22 years of his life. He sports an iPhone 3GS which rings non-stop. He jokes, “I am like the telephone switch board.” He moved to Kabul six years ago to work for the UN, then switched to work for a US State Department Justice Support Initiative, and then as an administrator for the International Medical Corps. But he likes his current job at the hospital most, because he sees the people he helps.

Zia says that the biggest problems with hospital are social. Patients fight with doctors, neglect health codes, and barge into Operating rooms during surgery. “They are unfamiliar with hospital conduct.”
*** READ ON FOR THE GRITTY DETAILS ***
Please forgive the current look, I have to clean up this formatting.
Nangahar Public Hospital Visit (01/04/11Â — 10AM — 3:30PM)
Lou and Peretz visited the hospital to inspect equipment, meet staff, and assess needs.
Met:
- Ahmed Zia Ahmedi, Hospital Administrator
- Dr. Baz Mohammad, Hospital Director
- Alhaj, Prof. Mohammad Ismail “Alam”, Chief of Medical Ward
- Nurse of Medical Ward
- Doctor from Surgical Ward
- Almas (stayed for first hour)
- Qahar, Internet Facilitator of Medical Faculty, accompanied us until lunch.
Places:
- Admin Offices
- Medical Ward — ICU/CCU
- Surgery Ward — Post Op Recovery Men/Women
- Equipmnent Storage
Equipment Inspected:
- Bed Side Patient Monitors — Philips SureSigns VM8
- 1 in Storage — missing cables — apparently Rotary and AI crew already know about this and are bringing the needed cables. Is this correct?
- Ed Myers — 1 unit in storage should not be a Philips Patient Monitor email indicates the locations — Maybe it shouldn’t, but it is: http://www.flickr.com/photos/49543096@N03/5327332655/ From the locations email vs what we have seen, this is probably the free standing one from the Operating Theater. We will make a point to track down cables. Then again, in the photo all of the cables appear to be there. We’ll figure out what to do with it and report back!
- 9 in Medical Ward (All working. Sticky electrodes — apparently HELBIG doesn’t work, but PLIA-CELL DIAGNOSTIC ones do work.)
- Ed Myers-Some of the ekg stickys are for the 12 lead EKG machine so this is true
- Is the 12 lead EKG in storage? We saw two GE ECG machines (see below)
- Ed Myers-Some of the ekg stickys are for the 12 lead EKG machine so this is true
- 2 in Surgial Ward (One missing the blood pressure cuff. They don’t have any    sticky  leads.)
- Ed Myers- ICU/CCU has supplies for entire hospital and they must share since this is where we put the supplies so the hospital would have a central supply room. This should help for accountability re ordering etc Great!
- Did not inspect 1 in Gynocology and 1 in Pediatrics, but reports are they are working.
- 1 in Storage — missing cables — apparently Rotary and AI crew already know about this and are bringing the needed cables. Is this correct?
- 2 Older Patient Monitors (Medical Ward) “Broken”
- First unit MEC-1000 missing fuse (“T1.6A” outside or “5TT 1.6A 250V ul” on old working fuse.) They bought replacement fuses, which do not work. This may be because they purchased a 10A fuse, which still fit the socket. I currently have the old broken fuse and the replacement fuse they got. Any ideas on where to look for replacements?
- Ed Myers- I left fuses for the Philips monitors they are T1.6amp, head nurse knows where they are they where left for eng Storrs. We only met him briefly then disappeared. Also left were memory sticks with latest software that i installed. These stick also contain manuals/guides. You might want to look at them if you have the time. > Great!
- Second unit GT9000 seems to work, but is missing cables. Appartently this is because the cables are now in Kabul with the person who is shopping for more cables. This is a good thing.
- First unit MEC-1000 missing fuse (“T1.6A” outside or “5TT 1.6A 250V ul” on old working fuse.) They bought replacement fuses, which do not work. This may be because they purchased a 10A fuse, which still fit the socket. I currently have the old broken fuse and the replacement fuse they got. Any ideas on where to look for replacements?
- 2 ECG Machines (Storage — awaiting deployment) — GE Mac 5000
- One battery (GE MAC PAC 18V 3500mAH NiMH, GEMS-IT P/N:900770–001) seems to be defective. Unit works when plugged into wall, but when unplugged, the charge holds for ~ one minute. We swapped batteries between units and confirmed that this is a battery rather than a unit/charger issue. If this cannot be locally sourced, one possibility would be for us to open up the battery case and replace the internal NiMH batteries with ones that we probably can purchase here.
- Any input?
- Second battery works fine. Both units are now in storage, awaiting distribution. Medical Ward wants one. Actually they want both.
- Brad says, one was shipped without connectors but connectors are coming.
- One battery (GE MAC PAC 18V 3500mAH NiMH, GEMS-IT P/N:900770–001) seems to be defective. Unit works when plugged into wall, but when unplugged, the charge holds for ~ one minute. We swapped batteries between units and confirmed that this is a battery rather than a unit/charger issue. If this cannot be locally sourced, one possibility would be for us to open up the battery case and replace the internal NiMH batteries with ones that we probably can purchase here.
- 1 BiliBlanket Transilluminator (Storage) — Which they thought was a broken UPS and now that they know what it is, are unsure what to do with. Apparently this is used in neonatal wards for infant light therapy (to treat/prevent jaundice) and as a transilluminator in helping locate veins for IV. We can explain this to the doctors, but perhaps this will require a training demonstration. MedWeb?
- 1 Ohmeda Medical Phototherapy (Storage) — Also for treating neonatal Jaundice — Missing bulb and internal cables. Apparently Rotary and AI crew is aware of this and will bring needed parts. Is this correct?
- Ed Myers- this is correct unit needs a new bulb it blew out wiring should be okay. Brad is more familiar.
- Almas and Qahar (the IT guy) said they know what to do with the part once they get it.
- Ed Myers- this is correct unit needs a new bulb it blew out wiring should be okay. Brad is more familiar.
- 1 Difibrillator (Storage) — “We have theoretical knowledge how to use it and think it works but we have not yet had a patient who has needed it.“ I neglected to inquire why it is in storage, rather than at a location where a patient might need it. This is an interesting point that they do not have patients that need it. Does it mean that by the time they get to hospital, they no longer need it? Would a training session be helpful to encourage its use? Medweb?
- Ed Myers- I am sure they will need it someday, no comment, it should always be plugged into power to keep battery charged and close to patients for when it is needed. It is a short period of time between V‑fib and death.. Dr Steve can comment
- We will make sure to relay this information. Where would be a good place to keep it?
- Ed Myers- I am sure they will need it someday, no comment, it should always be plugged into power to keep battery charged and close to patients for when it is needed. It is a short period of time between V‑fib and death.. Dr Steve can comment
Summary of Requests:
- Medical Ward wants more patient monitors. They have 15 beds. 9 new monitors. 2 old, under repair. Want 4 more. Actually they want 6 more new ones ;) This doesn’t need response. It’s just for the record.
- Medical Ward wants ultrasound machine (which the doctor called it a “doppler machine”.) The current one is located in Gynocology Ward. Zia suggested that it was too heavy to move and so it has remained in gynocolgy. Probably this is an internal issue of the hospital and not our issue, but nevertheless recorded. This doesn’t need a response. Just for the record.
- Medical Ward wants help getting new fuses for patient monitor. Solved
- Surgical Ward needs sticky electrodes for patient monitors. I suggested that they start by asking the Medical Ward to share. (They did not know the Medical Ward had any. Zia said he will assist with this.) Solved
- Surgical Ward needs a blood pressure cuff for a patient monitor which is missing one. (Did it go missing during installations?)
- Ed Myers- The ICU/CCU area has a cuff for this monitor Great!
- New MAC PAC battery for the GE MAC 5000 Portable ECG?
- Hospital Administration wants internet. They currently have intermittent internet. Zia said when it works it is very slow and it’s often out for up to a few weeks at a time. (Is it Fab Fi? They seemed to suggest so.) He stressed how important this is, “more important than anything else.” They have emails and things to look up, partient records, medical info, but often cannot do so. Zia says there is internet in MedWeb Room that Almas knows about, but that it is not shared around. Will ask Almas about this, but perhaps someone else knows about this also?
- It may be that new NATO funded internet which is going up at teaching hospital will cover them too. Anyone can confirm?
Recommendations:
It would be really convenient to have a Radio Shack in town, to grab fuses and such. It’s far less optimal to have to source things from far away, in terms of time, money and sustainablity. It would be good to source items locally. Perhaps we can help jump start a local distributor business by guaranteeing their inventory investment (say starting with good UPSs, fuses, EKG electrodes, …) their job will be to keep track of where to source such items when necessary and carry an inventory of the most frequently used items. Can you please help assess the merits of such an idea?
Ed Myers- divine intervention on may home from amsterdam the last night I met a Philips person in the hotel reception are who handles this part of the world. This is a great idea for a start up or see if this group is an opportunity that allready exist. I will send this email tonight. Thank you Ed, I will make sure to follow up.
Transport:
— IN: Salahudin (Mehrab’s nephew and his assistant at the Taj)
— OUT: Mr. Dawood, who says hello to all of the Rotary and AI crew he had transported previously!
We are having problems getting around and have to beg for rides. We would be more effective if we had a more reliable arrangement with a driver that we can call and pay to give us rides. Any suggestions?
***
Question to Fary — Is there yet another place where equipment is stored and not used? In a previous email you referred to “for example, US military purchased $450.000.00 worth of equipments sitting in the corner of room and dusting because they do not know how to use them.“ I was not able to locate this with questions alone. Also, according to your estimations which equipment do the doctors need training with (but will not admit it)? I could use some advice as to how to probe. Perhaps it is in the teaching hospital? We have met with Dr. Khan today but did not complete the inspection. “The person with the key” was not around. We are coming back on Saturday.
Question to Steve Brown — Qahar said you had a plan to make a Medical Library. Could you share some details of the project? I have brought many (and have access to more) ebook textbooks on different subjects (science, engineering, agriculture, ESL, etc.) and talked to Qahar about hosting this data on the local network at the Medical Faculty.
Idea — Can negotiate free PubMED access?